



Biblio du mois : Juillet 2018
 12 août 2018
12 août 2018
Et oui, le mois de Juillet a été chargé en émotion (pour rappel : la France est championne du monde de football ! ;-)) mais l’AJAR Paris vous livre une nouvelle biblio du mois pour continuer sur cet été 2018 de folie !
Au programme, de quoi débattre sur l’intérêt des PFC en pré-hospitalier, découdre l’intérêt de la PCT en infectiologie mais aussi des bienfaits du Café mais aussi la gestion du SDRA pédiatrique (PEP, APRICOT & co) !
Et surtout une étude comparative de l’intubation en réanimation vs en anesthésie… et oui il y a une différence significative …
On n’oubliera l’étude Bicar-ICU, les études sur les effets de la dexdetomedine sur la clairance de lactate ? sur le delirium post-AG ?
Avec un petit clin d’oeil à l’avenir avec du machine learning pour prédire l’insuffisance rénale aigue ! On vous prépare un évènement pour vous aider à traduire cela !


Suspicion d’infection respiratoire basse : Pas d’intérêt de la PCT pour guider l’antibiothérapie ?
N Engl J Med. 2018 Jul 19;379(3):236-249. doi: 10.1056/NEJMoa1802670. Epub 2018 May 20.
Procalcitonin-Guided Use of Antibiotics for Lower Respiratory Tract Infection.
Huang DT1, Yealy DM1, Filbin MR1, Brown AM1, Chang CH1, Doi Y1, Donnino MW1, Fine J1, Fine MJ1, Fischer MA1, Holst JM1, Hou PC1, Kellum JA1, Khan F1, Kurz MC1, Lotfipour S1, LoVecchio F1, Peck-Palmer OM1, Pike F1, Prunty H1, Sherwin RL1, Southerland L1, Terndrup T1, Weissfeld LA1, Yabes J1, Angus DC1; ProACT Investigators.
BACKGROUND:
The effect of procalcitonin-guided use of antibiotics on treatment for suspected lower respiratory tract infection is unclear.
METHODS:
In 14 U.S. hospitals with high adherence to quality measures for the treatment of pneumonia, we provided guidance for clinicians about national clinical practice recommendations for the treatment of lower respiratory tract infections and the interpretation of procalcitonin assays. We then randomly assigned patients who presented to the emergency department with a suspected lower respiratory tract infection and for whom the treating physician was uncertain whether antibiotic therapy was indicated to one of two groups: the procalcitonin group, in which the treating clinicians were provided with real-time initial (and serial, if the patient was hospitalized) procalcitonin assay results and an antibiotic use guideline with graded recommendations based on four tiers of procalcitonin levels, or the usual-care group. We hypothesized that within 30 days after enrollment the total antibiotic-days would be lower – and the percentage of patients with adverse outcomes would not be more than 4.5 percentage points higher – in the procalcitonin group than in the usual-care group.
RESULTS:
A total of 1656 patients were included in the final analysis cohort (826 randomly assigned to the procalcitonin group and 830 to the usual-care group), of whom 782 (47.2%) were hospitalized and 984 (59.4%) received antibiotics within 30 days. The treating clinician received procalcitonin assay results for 792 of 826 patients (95.9%) in the procalcitonin group (median time from sample collection to assay result, 77 minutes) and for 18 of 830 patients (2.2%) in the usual-care group. In both groups, the procalcitonin-level tier was associated with the decision to prescribe antibiotics in the emergency department. There was no significant difference between the procalcitonin group and the usual-care group in antibiotic-days (mean, 4.2 and 4.3 days, respectively; difference, -0.05 day; 95% confidence interval [CI], -0.6 to 0.5; P=0.87) or the proportion of patients with adverse outcomes (11.7% [96 patients] and 13.1% [109 patients]; difference, -1.5 percentage points; 95% CI, -4.6 to 1.7; P<0.001 for noninferiority) within 30 days.
CONCLUSIONS:
The provision of procalcitonin assay results, along with instructions on their interpretation, to emergency department and hospital-based clinicians did not result in less use of antibiotics than did usual care among patients with suspected lower respiratory tract infection. (Funded by the National Institute of General Medical Sciences; ProACT ClinicalTrials.gov number, NCT02130986 .).
Intérêt du plasma pré-hospitalier après traumatisme à risque de choc hémorragique ?
Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock.
Sperry JL1, Guyette FX1, Brown JB1, Yazer MH1, Triulzi DJ1, Early-Young BJ1, Adams PW1, Daley BJ1, Miller RS1, Harbrecht BG1, Claridge JA1, Phelan HA1, Witham WR1, Putnam AT1, Duane TM1, Alarcon LH1, Callaway CW1, Zuckerbraun BS1, Neal MD1, Rosengart MR1, Forsythe RM1, Billiar TR1, Yealy DM1, Peitzman AB1, Zenati MS1; PAMPer Study Group.
BACKGROUND:
After a person has been injured, prehospital administration of plasma in addition to the initiation of standard resuscitation procedures in the prehospital environment may reduce the risk of downstream complications from hemorrhage and shock. Data from large clinical trials are lacking to show either the efficacy or the risks associated with plasma transfusion in the prehospital setting.
METHODS:
To determine the efficacy and safety of prehospital administration of thawed plasma in injured patients who are at risk for hemorrhagic shock, we conducted a pragmatic, multicenter, cluster-randomized, phase 3 superiority trial that compared the administration of thawed plasma with standard-care resuscitation during air medical transport. The primary outcome was mortality at 30 days.
RESULTS:
A total of 501 patients were evaluated: 230 patients received plasma (plasma group) and 271 received standard-care resuscitation (standard-care group). Mortality at 30 days was significantly lower in the plasma group than in the standard-care group (23.2% vs. 33.0%; difference, -9.8 percentage points; 95% confidence interval, -18.6 to -1.0%; P=0.03). A similar treatment effect was observed across nine prespecified subgroups (heterogeneity chi-square test, 12.21; P=0.79). Kaplan-Meier curves showed an early separation of the two treatment groups that began 3 hours after randomization and persisted until 30 days after randomization (log-rank chi-square test, 5.70; P=0.02). The median prothrombin-time ratio was lower in the plasma group than in the standard-care group (1.2 [interquartile range, 1.1 to 1.4] vs. 1.3 [interquartile range, 1.1 to 1.6], P<0.001) after the patients’ arrival at the trauma center. No significant differences between the two groups were noted with respect to multiorgan failure, acute lung injury-acute respiratory distress syndrome, nosocomial infections, or allergic or transfusion-related reactions.
CONCLUSIONS:
In injured patients at risk for hemorrhagic shock, the prehospital administration of thawed plasma was safe and resulted in lower 30-day mortality and a lower median prothrombin-time ratio than standard-care resuscitation. (Funded by the U.S. Army Medical Research and Materiel Command; PAMPer ClinicalTrials.gov number, NCT01818427 .).
Revue sur les encéphalites aigues virales
Tyler, NEJM, 2018
https://www.nejm.org/doi/full/10.1056/NEJMra1708714?query=TOC
DOI: 10.1056/NEJMra1708714
![]()
Bicar-ICU : On tamponne pour passer le cap ?
Jaber et al., Lancet, 2018
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31080-8/fulltext
DOI: https://doi.org/10.1016/S0140-6736(18)31080-8
Background
Acute acidaemia is frequently observed during critical illness. Sodium bicarbonate infusion for the treatment of severe metabolic acidaemia is a possible treatment option but remains controversial, as no studies to date have examined its effect on clinical outcomes. Therefore, we aimed to evaluate whether sodium bicarbonate infusion would improve these outcomes in critically ill patients.
Methods
We did a multicentre, open-label, randomised controlled, phase 3 trial. Local investigators screened eligible patients from 26 intensive care units (ICUs) in France. We included adult patients (aged ≥18 years) who were admitted within 48 h to the ICU with severe acidaemia (pH ≤7·20, PaCO2 ≤45 mm Hg, and sodium bicarbonate concentration ≤20 mmol/L) and with a total Sequential Organ Failure Assessment score of 4 or more or an arterial lactate concentration of 2 mmol/L or more. We randomly assigned patients (1:1), by stratified randomisation with minimisation via a restricted web platform, to receive either no sodium bicarbonate (control group) or 4·2% of intravenous sodium bicarbonate infusion (bicarbonate group) to maintain the arterial pH above 7·30. Our protocol recommended that the volume of each infusion should be within the range of 125–250 mL in 30 min, with a maximum of 1000 mL within 24 h after inclusion. Randomisation criteria were stratified among three prespecified strata: age, sepsis status, and the Acute Kidney Injury Network (AKIN) score. The primary outcome was a composite of death from any cause by day 28 and the presence of at least one organ failure at day 7. All analyses were done on data from the intention-to-treat population, which included all patients who underwent randomisation. This study is registered with ClinicalTrials.gov, number NCT02476253.
Findings
Between May 5, 2015, and May 7, 2017, we enrolled 389 patients into the intention-to-treat analysis in the overall population (194 in the control group and 195 in the bicarbonate group). The primary outcome occurred in 138 (71%) of 194 patients in the control group and 128 (66%) of 195 in the bicarbonate group (absolute difference estimate −5·5%, 95% CI −15·2 to 4·2; p=0·24). The Kaplan-Meier method estimate of the probability of survival at day 28 between the control group and bicarbonate group was not significant (46% [95% CI 40–54] vs 55% [49–63]; p=0·09. In the prespecified AKIN stratum of patients with a score of 2 or 3, the Kaplan-Meier method estimate of survival by day 28 between the control group and bicarbonate group was significant (63% [95% CI 52–72] vs 46% [35–55]; p=0·0283). Metabolic alkalosis, hypernatraemia, and hypocalcaemia were observed more frequently in the bicarbonate group than in the control group, with no life-threatening complications reported.
Interpretation
In patients with severe metabolic acidaemia, sodium bicarbonate had no effect on the primary composite outcome. However, sodium bicarbonate decreased the primary composite outcome and day 28 mortality in the a-priori defined stratum of patients with acute kidney injury.
Avancées avec la e-médecine périopératoire personnalisée ?
van der Meij, et al., Lancet, 2018
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31113-9/fulltext
DOI: https://doi.org/10.1016/S0140-6736(18)31113-9
Background
Instructing and guiding patients after surgery is essential for successful recovery. However, the time that health-care professionals can spend with their patients postoperatively has been reduced because of efficiency-driven, shortened hospital stays. We evaluated the effect of a personalised e-health-care programme on return to normal activities after surgery.
Methods
A multicentre, single-blind, randomised controlled trial was done at seven teaching hospitals in the Netherlands. Patients aged 18–75 years who were scheduled for laparoscopic cholecystectomy, inguinal hernia surgery, or laparoscopic adnexal surgery for a benign indication were recruited. An independent researcher randomly allocated participants to either the intervention or control group using computer-based randomisation lists, with stratification by sex, type of surgery, and hospital. Participants in the intervention group had access to a perioperative, personalised, e-health-care programme, which managed recovery expectations and provided postoperative guidance tailored to the patient. The control group received usual care and access to a placebo website containing standard general recovery advice. Participants were unaware of the study hypothesis and were asked to complete questionnaires at five timepoints during the 6-month period after surgery. The primary outcome was time between surgery and return to normal activities, measured using personalised patient-reported outcome measures. Intention-to-treat and per-protocol analyses were done. This trial is registered in the Netherlands National Trial Register, number NTR4699.
Findings
Between Aug 24, 2015, and Aug 12, 2016, 344 participants were enrolled and randomly allocated to either the intervention (n=173) or control (n=171) group. 14 participants (4%) were lost to follow-up, with 330 participants included in the primary outcome analysis. Median time until return to normal activities was 21 days (95% CI 17–25) in the intervention group and 26 days (20–32) in the control group (hazard ratio 1·38, 95% CI 1·09–1·73; p=0·007). Complications did not differ between groups.
Interpretation
A personalised e-health intervention after abdominal surgery speeds up the return to normal activities compared with usual care. Implementation of this e-health programme is recommended in patients undergoing intermediate-grade abdominal, gynaecological, or general surgical procedures.
PFC pré-hospitalier : NS
Moore et al., Lancet, 2018
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31553-8/fulltext
DOI: https://doi.org/10.1016/S0140-6736(18)31553-8
Background
Plasma is integral to haemostatic resuscitation after injury, but the timing of administration remains controversial. Anticipating approval of lyophilised plasma by the US Food and Drug Administration, the US Department of Defense funded trials of prehospital plasma resuscitation. We investigated use of prehospital plasma during rapid ground rescue of patients with haemorrhagic shock before arrival at an urban level 1 trauma centre.
Methods
The Control of Major Bleeding After Trauma Trial was a pragmatic, randomised, single-centre trial done at the Denver Health Medical Center (DHMC), which houses the paramedic division for Denver city. Consecutive trauma patients in haemorrhagic shock (defined as systolic blood pressure [SBP] ≤70 mm Hg or 71–90 mm Hg plus heart rate ≥108 beats per min) were assessed for eligibility at the scene of the injury by trained paramedics. Eligible patients were randomly assigned to receive plasma or normal saline (control). Randomisation was achieved by preloading all ambulances with sealed coolers at the start of each shift. Coolers were randomly assigned to groups 1:1 in blocks of 20 according to a schedule generated by the research coordinators. If the coolers contained two units of frozen plasma, they were defrosted in the ambulance and the infusion started. If the coolers contained a dummy load of frozen water, this indicated allocation to the control group and saline was infused. The primary endpoint was mortality within 28 days of injury. Analyses were done in the as-treated population and by intention to treat. This trial is registered with ClinicalTrials.gov, number NCT01838863.
Findings
From April 1, 2014, to March 31, 2017, paramedics randomly assigned 144 patients to study groups. The as-treated analysis included 125 eligible patients, 65 received plasma and 60 received saline. Median age was 33 years (IQR 25–47) and median New Injury Severity Score was 27 (10–38). 70 (56%) patients required blood transfusions within 6 h of injury. The groups were similar at baseline and had similar transport times (plasma group median 19 min [IQR 16–23] vs control 16 min [14–22]). The groups did not differ in mortality at 28 days (15% in the plasma group vs 10% in the control group, p=0·37). In the intention-to-treat analysis, we saw no significant differences between the groups in safety outcomes and adverse events. Due to the consistent lack of differences in the analyses, the study was stopped for futility after 144 of 150 planned enrolments.
Interpretation
During rapid ground rescue to an urban level 1 trauma centre, use of prehospital plasma was not associated with survival benefit. Blood products might be beneficial in settings with longer transport times, but the financial burden would not be justified in an urban environment with short distances to mature trauma centres.
![]()
Musculation précoce en réanimation : pas facile !
Importance Early in-bed cycling and electrical muscle stimulation may improve the benefits of rehabilitation in patients in the intensive care unit (ICU).
Objective To investigate whether early in-bed leg cycling plus electrical stimulation of the quadriceps muscles added to standardized early rehabilitation would result in greater muscle strength at discharge from the ICU.
Design, Setting, and Participants Single-center, randomized clinical trial enrolling critically ill adult patients at 1 ICU within an 1100-bed hospital in France. Enrollment lasted from July 2014 to June 2016 and there was a 6-month follow-up, which ended on November 24, 2016.
Interventions Patients were randomized to early in-bed leg cycling plus electrical stimulation of the quadriceps muscles added to standardized early rehabilitation (n = 159) or standardized early rehabilitation alone (usual care) (n = 155).
Main Outcomes and Measures The primary outcome was muscle strength at discharge from the ICU assessed by physiotherapists blinded to treatment group using the Medical Research Council grading system (score range, 0-60 points; a higher score reflects better muscle strength; minimal clinically important difference of 4 points). Secondary outcomes at ICU discharge included the number of ventilator-free days and ICU Mobility Scale score (range, 0-10; a higher score reflects better walking capability). Functional autonomy and health-related quality of life were assessed at 6 months.
Results Among 314 randomized patients, 312 (mean age, 66 years; women, 36%; receiving mechanical ventilation at study inclusion, 78%) completed the study and were included in the analysis. The median global Medical Research Council score at ICU discharge was 48 (interquartile range [IQR], 29 to 58) in the intervention group and 51 (IQR, 37 to 58) in the usual care group (median difference, −3.0 [95% CI, −7.0 to 2.8]; P = .28). The ICU Mobility Scale score at ICU discharge was 6 (IQR, 3 to 9) in both groups (median difference, 0 [95% CI, −1 to 2]; P = .52). The median number of ventilator-free days at day 28 was 21 (IQR, 6 to 25) in the intervention group and 22 (IQR, 10 to 25) in the usual care group (median difference, 1 [95% CI, −2 to 3]; P = .24). Clinically significant events occurred during mobilization sessions in 7 patients (4.4%) in the intervention group and in 9 patients (5.8%) in the usual care group. There were no significant between-group differences in the outcomes assessed at 6 months.
Conclusions and Relevance In this single-center randomized clinical trial involving patients admitted to the ICU, adding early in-bed leg cycling exercises and electrical stimulation of the quadriceps muscles to a standardized early rehabilitation program did not improve global muscle strength at discharge from the ICU.
Des probiotiques pour prévenir les infections à Clostridium difficile chez les patients sous antibiotiques ?
Pas tous égaux face aux bienfaits du café ?
Importance Prospective cohorts in North America, Europe, and Asia show consistent inverse associations between coffee drinking and mortality, including deaths from cardiovascular disease and some cancers. However, concerns about coffee, particularly among people with common genetic polymorphisms affecting caffeine metabolism and among those drinking more than 5 cups per day, remain.
Objective To evaluate associations of coffee drinking with mortality by genetic caffeine metabolism score.
Design, Setting, and Participants The UK Biobank is a population-based study that invited approximately 9.2 million individuals from across the United Kingdom to participate. We used baseline demographic, lifestyle, and genetic data form the UK Biobank cohort, with follow-up beginning in 2006 and ending in 2016, to estimate hazard ratios (HRs) for coffee intake and mortality, using multivariable-adjusted Cox proportional hazards models. We investigated potential effect modification by caffeine metabolism, defined by a genetic score of previously identified polymorphisms in AHR, CYP1A2, CYP2A6, and POR that have an effect on caffeine metabolism. Of the 502 641 participants who consented with baseline data, we included those who were not pregnant and had complete data on coffee intake and smoking status (n = 498 134).
Exposures Total, ground, instant, and decaffeinated coffee intake.
Main Outcomes and Measures All-cause and cause-specific mortality.
Results The mean age of the participants was 57 years (range, 38-73 years); 271 019 (54%) were female, and 387 494 (78%) were coffee drinkers. Over 10 years of follow-up, 14 225 deaths occurred. Coffee drinking was inversely associated with all-cause mortality. Using non–coffee drinkers as the reference group, HRs for drinking less than 1, 1, 2 to 3, 4 to 5, 6 to 7, and 8 or more cups per day were 0.94 (95% CI, 0.88-1.01), 0.92 (95% CI, 0.87-0.97), 0.88 (95% CI, 0.84-0.93), 0.88 (95% CI, 0.83-0.93), 0.84 (95% CI, 0.77-0.92), and 0.86 (95% CI, 0.77-0.95), respectively. Similar associations were observed for instant, ground, and decaffeinated coffee, across common causes of death, and regardless of genetic caffeine metabolism score. For example, the HRs for 6 or more cups per day ranged from 0.70 (95% CI, 0.53-0.94) to 0.92 (95% CI, 0.78-1.10), with no evidence of effect modification across strata of caffeine metabolism score (P = .17 for heterogeneity).
Conclusions and Relevance Coffee drinking was inversely associated with mortality, including among those drinking 8 or more cups per day and those with genetic polymorphisms indicating slower or faster caffeine metabolism. These findings suggest the importance of noncaffeine constituents in the coffee-mortality association and provide further reassurance that coffee drinking can be a part of a healthy diet.
Enfin des preuves pour l’acupuncture ?
https://jamanetwork.com/journals/jama/article-abstract/2687355
Importance Musculoskeletal symptoms are the most common adverse effects of aromatase inhibitors and often result in therapy discontinuation. Small studies suggest that acupuncture may decrease aromatase inhibitor–related joint symptoms.
Objective To determine the effect of acupuncture in reducing aromatase inhibitor–related joint pain.
Design, Setting, and Patients Randomized clinical trial conducted at 11 academic centers and clinical sites in the United States from March 2012 to February 2017 (final date of follow-up, September 5, 2017). Eligible patients were postmenopausal women with early-stage breast cancer who were taking an aromatase inhibitor and scored at least 3 on the Brief Pain Inventory Worst Pain (BPI-WP) item (score range, 0-10; higher scores indicate greater pain).
Interventions Patients were randomized 2:1:1 to the true acupuncture (n = 110), sham acupuncture (n = 59), or waitlist control (n = 57) group. True acupuncture and sham acupuncture protocols consisted of 12 acupuncture sessions over 6 weeks (2 sessions per week), followed by 1 session per week for 6 weeks. The waitlist control group did not receive any intervention. All participants were offered 10 acupuncture sessions to be used between weeks 24 and 52.
Main Outcomes and Measures The primary end point was the 6-week BPI-WP score. Mean 6-week BPI-WP scores were compared by study group using linear regression, adjusted for baseline pain and stratification factors (clinically meaningful difference specified as 2 points).
Results Among 226 randomized patients (mean [SD] age, 60.7 [8.6] years; 88% white; mean [SD] baseline BPI-WP score, 6.6 [1.5]), 206 (91.1%) completed the trial. From baseline to 6 weeks, the mean observed BPI-WP score decreased by 2.05 points (reduced pain) in the true acupuncture group, by 1.07 points in the sham acupuncture group, and by 0.99 points in the waitlist control group. The adjusted difference for true acupuncture vs sham acupuncture was 0.92 points (95% CI, 0.20-1.65; P = .01) and for true acupuncture vs waitlist control was 0.96 points (95% CI, 0.24-1.67; P = .01). Patients in the true acupuncture group experienced more grade 1 bruising compared with patients in the sham acupuncture group (47% vs 25%; P = .01).
Conclusions and Relevance Among postmenopausal women with early-stage breast cancer and aromatase inhibitor–related arthralgias, true acupuncture compared with sham acupuncture or with waitlist control resulted in a statistically significant reduction in joint pain at 6 weeks, although the observed improvement was of uncertain clinical importance.

Dialyse précoce ou tardive dans le choc septique et le SDRA ?
Gaudry et al., ICM, 2018
(analyse secondaire de l’étude AKIKI)
https://www.atsjournals.org/doi/full/10.1164/rccm.201706-1255OC
https://doi.org/10.1164/rccm.201706-1255OC
Rationale: The optimal strategy for initiation of renal replacement therapy (RRT) in patients with severe acute kidney injury in the context of septic shock and acute respiratory distress syndrome (ARDS) is unknown.
Objectives: To examine the effect of an early compared with a delayed RRT initiation strategy on 60-day mortality according to baseline sepsis status, ARDS status, and severity.
Methods: Post hoc analysis of the AKIKI (Artificial Kidney Initiation in Kidney Injury) trial.
Measurements and Main Results: Subgroups were defined according to baseline characteristics: sepsis status (Sepsis-3 definition), ARDS status (Berlin definition), Simplified Acute Physiology Score 3 (SAPS 3), and Sepsis-related Organ Failure Assessment (SOFA). Of 619 patients, 348 (56%) had septic shock and 207 (33%) had ARDS. We found no significant influence of the baseline sepsis status (P = 0.28), baseline ARDS status (P = 0.94), and baseline severity scores (P = 0.77 and P = 0.46 for SAPS 3 and SOFA, respectively) on the comparison of 60-day mortality according to RRT initiation strategy. A delayed RRT initiation strategy allowed 45% of patients with septic shock and 46% of patients with ARDS to escape RRT. Urine output was higher in the delayed group. Renal function recovery occurred earlier with the delayed RRT strategy in patients with septic shock or ARDS (P < 0.001 and P = 0.003, respectively). Time to successful extubation in patients with ARDS was not affected by RRT strategy (P = 0.43).
Conclusions: Early RRT initiation strategy was not associated with any improvement of 60-day mortality in patients with severe acute kidney injury and septic shock or ARDS. Unnecessary and potentially risky procedures might often be avoided in these fragile populations.
Même niveau de PEP dans le SDRA pour l’enfant ?
https://doi.org/10.1164/rccm.201707-1404OC
Rationale: The ARDS Network (ARDSNet) used a positive end-expiratory pressure (PEEP)/FiO2 model in many studies. In general, pediatric intensivists use less PEEP and higher FiO2 than this model.
Objectives: To evaluate whether children managed with PEEP lower than recommended by the ARDSNet PEEP/FiO2 model had higher mortality.
Methods: This was a multicenter, retrospective analysis of patients with pediatric acute respiratory distress syndrome (PARDS) managed without a formal PEEP/FiO2 protocol. Four distinct datasets were combined for analysis. We extracted time-matched PEEP/FiO2 values, calculating the difference between PEEP level and the ARDSNet-recommended PEEP level for a given FiO2. We analyzed the median difference over the first 24 hours of PARDS diagnosis against ICU mortality and adjusted for confounding variables, effect modifiers, or factors that may have affected the propensity to use lower PEEP.
Measurements and Main Results: Of the 1,134 patients with PARDS, 26.6% were managed with lower PEEP relative to the amount of FiO2 recommended by the ARDSNet protocol. Patients managed with lower PEEP experienced higher mortality than those who were managed with PEEP levels in line with or higher than recommended by the protocol (P < 0.001). After adjustment for hypoxemia, inotropes, comorbidities, severity of illness, ventilator settings, nitric oxide, and dataset, PEEP lower than recommended by the protocol remained independently associated with higher mortality (odds ratio, 2.05; 95% confidence interval, 1.32–3.17). Findings were similar after propensity-based covariate adjustment (odds ratio, 2.00; 95% confidence interval, 1.24–3.22).
Conclusions: Patients with PARDS managed with lower PEEP relative to FiO2 than recommended by the ARDSNet model had higher mortality. Clinical trials targeting PEEP management in PARDS are needed.

L’anesthésie générale altère-t-elle les fonctions cognitives ?
Background
The link between exposure to general anaesthesia and surgery (exposure) and cognitive decline in older adults is debated. We hypothesised that it is associated with cognitive decline.
Methods
We analysed the longitudinal cognitive function trajectory in a cohort of older adults. Models assessed the rate of change in cognition over time, and its association with exposure to anaesthesia and surgery. Analyses assessed whether exposure in the 20 yr before enrolment is associated with cognitive decline when compared with those unexposed, and whether post-enrolment exposure is associated with a change in cognition in those unexposed before enrolment.
Results
We included 1819 subjects with median (25th and 75th percentiles) follow-up of 5.1 (2.7–7.6) yr and 4 (3–6) cognitive assessments. Exposure in the previous 20 yr was associated with a greater negative slope compared with not exposed (slope: –0.077 vs –0.059; difference: –0.018; 95% confidence interval: –0.032, –0.003; P=0.015). Post-enrolment exposure in those previously unexposed was associated with a change in slope after exposure (slope: –0.100 vs –0.059 for post-exposure vs pre-exposure, respectively; difference: –0.041; 95% confidence interval: –0.074, –0.008; P=0.016). Cognitive impairment could be attributed to declines in memory and attention/executive cognitive domains.
Conclusions
In older adults, exposure to general anaesthesia and surgery was associated with a subtle decline in cognitive z-scores. For an individual with no prior exposure and with exposure after enrolment, the decline in cognitive function over a 5 yr period after the exposure would be 0.2 standard deviations more than the expected decline as a result of ageing. This small cognitive decline could be meaningful for individuals with already low baseline cognition.
Mieux cibler la place des bêta-bloquants en chirurgie non cardiaque
M.E. Jørgensen, et al., BJA, 2018
Gestion des voies aériennes en anesthésie pédiatrique
Background
Critical respiratory events are common in children in the peri-anaesthetic period and are caused by airway and ventilation management difficulties. We aimed to analyse current European paediatric airway management practices and identify the incidence and potential consequences of difficult airway management.
Methods
We performed a secondary analysis of airway and ventilation management details of the European multicentre observational trial (Anaesthesia PRactice in Children Observational Trial, APRICOT) of children from birth to 15 yr of age. The primary endpoint was the incidence of difficult airway management. Secondary endpoints were the associations between difficult airway management, known pre-existing respiratory risk factors, and the occurrence of critical respiratory events.
Results
Details for 31 024 anaesthetic procedures were available for analysis. Three or more tracheal intubation attempts were necessary in 120 children (0.9%) and in 40 children (0.4%) for supraglottic airways insertions. The incidence (95% confidence interval) for failed tracheal intubation and failed supraglottic airway insertions was 8/10 000 (0.08%; 0.03–0.13%) and 8.2/10 000 (0.08%; 0.03–0.14%) children, respectively. Difficulties in securing the airway increased the risk for a critical respiratory event for tracheal tube (2.1; 1.3–3.4) and supraglottic airway (4.3; 1.9–9.9) placement. History of pre-existing respiratory risk factors was significantly associated with critical respiratory events independently of the airway device used.
Conclusions
Airway management practices vary widely across Europe. Multiple airway device insertion attempts and pre-existing respiratory risk factors increase the likelihood of critical respiratory events in children and require further stratification during preoperative assessment and planning. This study highlights areas where education, research, and training may improve perioperative care.
Place à l’écho pour la pose de VVP !
(revue systématique et méta-analyse)
Le lactate prédictif de transfusion massive dans l’hémorragie du post-partum ?
Méta-analyse sur le dexmedetomidine et le delirium post-anesthésie générale
Duan at al., BJA, 2018
https://bjanaesthesia.org/article/S0007-0912(18)30447-1/fulltext

Méta-analyse sur la nutrition entérale précoce en réanimation
doi: 10.1097/CCM.0000000000003152
Un algorithme pour prédire l’insuffisance rénale aiguë en réanimation
Koyner, et al., CCM, 2018
https://journals.lww.com/ccmjournal/Fulltext/2018/07000/The_Development_of_a_Machine_Learning_Inpatient.5.aspx
doi: 10.1097/CCM.0000000000003123
Objectives: To develop an acute kidney injury risk prediction model using electronic health record data for longitudinal use in hospitalized patients.
Design: Observational cohort study.
Setting: Tertiary, urban, academic medical center from November 2008 to January 2016.
Patients: All adult inpatients without pre-existing renal failure at admission, defined as first serum creatinine greater than or equal to 3.0 mg/dL, International Classification of Diseases, 9th Edition, code for chronic kidney disease stage 4 or higher or having received renal replacement therapy within 48 hours of first serum creatinine measurement.
Interventions: None.
Measurements and Main Results: Demographics, vital signs, diagnostics, and interventions were used in a Gradient Boosting Machine algorithm to predict serum creatinine–based Kidney Disease Improving Global Outcomes stage 2 acute kidney injury, with 60% of the data used for derivation and 40% for validation. Area under the receiver operator characteristic curve (AUC) was calculated in the validation cohort, and subgroup analyses were conducted across admission serum creatinine, acute kidney injury severity, and hospital location. Among the 121,158 included patients, 17,482 (14.4%) developed any Kidney Disease Improving Global Outcomes acute kidney injury, with 4,251 (3.5%) developing stage 2. The AUC (95% CI) was 0.90 (0.90–0.90) for predicting stage 2 acute kidney injury within 24 hours and 0.87 (0.87–0.87) within 48 hours. The AUC was 0.96 (0.96–0.96) for receipt of renal replacement therapy (n = 821) in the next 48 hours. Accuracy was similar across hospital settings (ICU, wards, and emergency department) and admitting serum creatinine groupings. At a probability threshold of greater than or equal to 0.022, the algorithm had a sensitivity of 84% and a specificity of 85% for stage 2 acute kidney injury and predicted the development of stage 2 a median of 41 hours (interquartile range, 12–141 hr) prior to the development of stage 2 acute kidney injury.
Conclusions: Readily available electronic health record data can be used to predict impending acute kidney injury prior to changes in serum creatinine with excellent accuracy across different patient locations and admission serum creatinine. Real-time use of this model would allow early interventions for those at high risk of acute kidney injury.
![]()
Hémofiltration à haut volume précoce chez les (très) grands brulés pour épurer les mauvaises humeurs
o_O
Early application of continuous high-volume haemofiltration can reduce sepsis and improve the prognosis of patients with severe burns
Bo You, Yu Long Zhang, Gao Xing Luo, Yong Ming Dang, Bei Jiang, Guang Tao Huang, Xin Zhu Liu, Zi Chen Yang, Yu Chen, Jing Chen, Zhi Qiang Yuan, Su Peng Yin†and Yi Zhi Peng†
https://ccforum.biomedcentral.com/articles/10.1186/s13054-018-2095-9
Background
In the early stage of severe burn, patients often exhibit a high level of inflammatory mediators in blood and are likely to develop sepsis. High-volume haemofiltration (HVHF) can eliminate these inflammatory mediators. We hypothesised that early application of HVHF may be beneficial in reducing sepsis and improving the prognosis of patients with severe burns.
Methods
Adults patients with burns ≥ 50% total burn surface area (TBSA) and in whom the sum of deep partial and full-thickness burn areas was ≥ 30% were enrolled in this randomised prospective study, and they were divided into control (41 cases) and HVHF (41 cases) groups. Patients in the control group received standard management for major burns, whereas the HVHF group additionally received HVHF treatment (65 ml/kg/h for 3 consecutive days) within 3 days after burn. The incidence of sepsis and mortality, some laboratory data, levels of inflammatory cytokines in the blood, HLA-DR expression on CD14+ peripheral blood monocytes, the proportion of CD25+Foxp3+ in CD4+ T lymphocytes, and the counts of CD3+, CD4+ and CD8+ T lymphocytes were recorded within 28 days post-burn.
Results
The incidence of sepsis, septic shock and duration of vasopressor treatment were decreased significantly in the HVHF group. In addition, in the subgroup of patients with burns ≥ 80% TBSA, the 90-day mortality showed significant decreases in the HVHF group. The ratio of arterial oxygen partial pressure to the fraction of inspiration oxygen was improved after HVHF treatment. In the patients who received HVHF treatment, the blood levels of inflammatory cytokines, including tumour necrosis factor-α, interleukin (IL)-1β, IL-6 and IL-8, as well as the blood level of procalcitonin were found to be lower than in the control group. Moreover, higher HLA-DR expression on CD14+ monocytes and a lower proportion of CD25+Foxp3+ in CD4+ T lymphocytes were observed in the patients in the HVHF group.
Conclusions
Early application of HVHF benefits patients with severe burns, especially for those with a greater burn area (≥ 80% TBSA), decreasing the incidence of sepsis and mortality. This effect may be attributed to its early clearance of inflammatory mediators and the recovery of the patient’s immune status.
Péritonites post-opératoires : Pas d’augmentation de la morbi-mortalité chez les patients bactériémiques
Clinical characteristics and prognosis of bacteraemia during postoperative intra-abdominal infections
Adel Alqarni, Elie Kantor, Nathalie Grall, Sebastien Tanaka, Nathalie Zappella, Mathieu Godement, Lara Ribeiro-Parenti, Alexy Tran-Dinh and Philippe Montravers
https://ccforum.biomedcentral.com/articles/10.1186/s13054-018-2099-5
Background
Bloodstream infections of abdominal origin are usually associated with poor prognosis. We assessed the clinical and microbiological characteristics of critically ill patients admitted to the intensive care unit (ICU) for postoperative intra-abdominal infection (PIAI) and analysed the influence of bacteraemia on their outcome.
Methods
All consecutive PIAI patients admitted to the ICU between 1999 and 2014 were prospectively analysed. Bacteraemic patients (at least one positive blood culture in the 24 h preceding/following surgery) were compared with non-bacteraemic patients. Demographic characteristics, underlying disease, severity scores at the time of reoperation, microbiological results, therapeutic management, outcome, and survival were recorded. Results are expressed as median (interquartile range (IQR)) or proportions.
Results
Overall, 343 patients (54% male, 62 (49–73) years old) with PIAI were analysed, including 64 (19%) bacteraemic patients. Immunosuppression and cancer were more frequent in bacteraemic patients (p < 0.001 in both cases). No difference between groups was observed for the characteristics of initial surgery. Time to reoperation, site, and cause of PIAI were similar in both groups. At the time of reoperation, Sequential Organ Failure Assessment (SOFA) score was higher in bacteraemic patients (8 (6–10) versus 7 (4–10); p < 0.05). A predominance of Gram-positive (34%) and Gram-negative (47%) bacteria were recovered from blood cultures (polymicrobial bacteraemia in 9 (14%) patients and bacteraemia involving multidrug-resistant organisms in 14 (22%) patients). In multivariate analysis, risk factors for bacteraemia were immunosuppression or cancer, high SOFA score, and E. coli in peritoneal samples. Bacteraemia did not impact the management (with similar results for the adequacy of antibiotic therapy, anti-infective agents used, de-escalation or duration of therapy in both groups). Neither hospital mortality nor morbidity criteria differed between groups. Risk factors for mortality in multivariate analysis were urgent initial surgery, high Simplified Acute Physiology Score (SAPS) II score and documented antifungal therapy, but not perioperative bacteraemia.
Conclusions
In this ICU population, bacteraemia did not change the overall management of patients with PIAI. Our data suggest that bacteraemic patients do not require a specific management.
Revue et méta-analyse sur le syndrome compartimental abdominal : la laparotomie décompressive améliore l’hémodynamique et l’hématose
Effect of decompressive laparotomy on organ function in patients with abdominal compartment syndrome: a systematic review and meta-analysis
Lana Van Damme and Jan J. De Waele
https://ccforum.biomedcentral.com/articles/10.1186/s13054-018-2103-0
Critical Care201822:179
https://doi.org/10.1186/s13054-018-2103-0
Background
Decompressive laparotomy has been advised as potential treatment for abdominal compartment syndrome (ACS) when medical management fails; yet, the effect on parameters of organ function differs markedly in the published literature. In this study, we sought to investigate the effect of decompressive laparotomy on intra-abdominal pressure and organ function in critically ill adult and pediatric patients with ACS, specifically focusing on hemodynamic, respiratory, and kidney function and outcome.
Methods
A systematic review and meta-analysis of the literature was performed. Articles reporting data on intra-abdominal pressure (IAP), hemodynamic (mean arterial pressures [MAP], central venous pressure [CVP], cardiac index [CI], heart rate [HR], systemic vascular resistance index [SVRI] and/or pulmonary capillary wedge pressure [PCWP]), respiratory (positive end-expiratory pressure [PEEP], peak inspiratory pressure [PIP] and/or ratio of partial pressure arterial oxygen and fraction of inspired oxygen [P/F ratio]), and/or urinary output (UO) following decompressive laparotomy were analyzed.
Results
A total of 15 articles were included; 3 included children only (aged 18 years or younger). Of the 286 patients who were included, 49.7% had primary ACS. The baseline mean IAP in adults decreased with an average of 18.2 ± 6.5 mmHg following decompression, from 31.7 ± 6.4 mmHg to 13.5 ± 3.0 mmHg. There was a decrease in HR (12.2 ± 9.5 beats/min; p = 0.04), CVP (4.6 ± 2.3 mmHg; p = 0.022), PCWP (5.8 ± 2.3 mmHg; p = 0.029), and PIP (10.1 ± 3.9 cmH2O; p < 0.001) and a mean increase in P/F ratio (70.4 ± 49.4; p < 0.001) and UO (95.3 ± 105.3 ml/h; p < 0.001). In children, there was a significant increase in MAP (20.0 ± 2.3 mmHg; p = 0.006), P/F ratio (238.2; p < 0.001), and UO (2.88 ± 0.64 ml/kg/h; p < 0.001) and a decrease in CVP (7 mmHg; p = 0.016) and PIP (9.9 cmH2O; p = 0.002). The overall mortality rate was 49.7% in adults and 60.8% in children following decompressive laparotomy.
Conclusions
Decompressive laparotomy resulted in a significantly lower IAP and had beneficial effects on hemodynamic, respiratory, and renal parameters. Mortality after decompressive laparotomy remains high in both adults and children.
Méta-analyse sur l’association Corticoïdes et Neuropathie de réanimation
Tao Yang†,et al., Critical Care 2018
https://ccforum.biomedcentral.com/articles/10.1186/s13054-018-2111-0
La sédation avec la dexmedetomidine est associée à une meilleure clairance du lactate
Effect of Dexmedetomidine on Lactate Clearance in Patients With Septic Shock: A Subanalysis of a Multicenter Randomized Controlled Trial
Miyamoto, Kyohei*; Nakashima, Tsuyoshi*; Shima, Nozomu*; Kato, Seiya*; Ueda, Kentaro*; Kawazoe, Yu†; Ohta, Yoshinori‡; Morimoto, Takeshi§; Yamamura, Hitoshi¶ on behalf of DESIRE Trial Investigators
doi: 10.1097/SHK.0000000000001055
ABSTRACT Lactate clearance is useful to guide initial resuscitation of patients with septic shock. We conducted this study to evaluate whether dexmedetomidine increases lactate clearance in patients with septic shock. This was a randomized controlled trial that involved a post hoc subgroup analysis. Adult patients with septic shock under ventilation were randomized to receive sedation strategy with or without dexmedetomidine (60 in the dexmedetomidine and 51 in the nondexmedetomidine groups). The primary outcome was the lactate clearance at 6 h, defined as the percent decrease in lactate from randomization to 6 h after. The median Acute Physiology and Chronic Health Evaluation II score was 25 (interquartile range 19–31). The median serum lactate value at randomization was lower in the dexmedetomidine group than in the nondexmedetomidine group (4.0 mmol/L vs. 4.8 mmol/L; P = 0.053). The lactate clearance at 6 h was higher in the dexmedetomidine group, although this was not statistically significant (23.3 ± 29.8 vs. 11.1 ± 54.4, mean difference 12.2, 95% confidence interval (CI), –4.4 to 28.8). After adjusting for the lactate level at randomization, lactate clearance at 6 h was significantly higher in the dexmedetomidine group (adjusted mean difference 18.5, 95% CI, 2.2–34.9). There was no statistically significant difference in the 28-day mortality between the dexmedetomidine and the nondexmedetomidine groups (13 [22%] vs. 18 [35%] patients, P = 0.11). In conclusion, among mechanically ventilated patients with septic shock, sedation with dexmedetomidine resulted in increased lactate clearance compared with sedation without dexmedetomidine.
Mécanisme d’action de l’adrecizumab : nouvelle immunothérapie du sepsis ?
Vascular Effects of Adrenomedullin and the Anti-Adrenomedullin Antibody Adrecizumab in Sepsis
Geven, Christopher*,†; Bergmann, Andreas‡; Kox, Matthijs*,†; Pickkers, Peter*,†
Shock: August 2018 – Volume 50 – Issue 2 – p 132–140
doi: 10.1097/SHK.0000000000001103
Review Article
ABSTRACT Sepsis remains a major scientific and medical challenge, for which, apart from significant refinements in supportive therapy, treatment has barely changed over the last few decades. During sepsis, both vascular tone and vascular integrity are compromised, and contribute to the development of shock. The free circulating peptide adrenomedullin (ADM) is involved in the regulation of the endothelial barrier function and tone of blood vessels. Several animal studies have shown that ADM administration improves outcome of sepsis. However, in higher dosages, ADM administration may cause hypotension, limiting its clinical applicability. Moreover, ADM has a very short half-life and easily adheres to surfaces, further hampering its clinical use. The non-neutralizing anti-ADM antibody Adrecizumab (HAM8101) which causes a long-lasting increase of plasma ADM has shown promising results in animal models of systemic inflammation and sepsis; it reduced inflammation, attenuated vascular leakage, and improved hemodynamics, kidney function, and survival. Combined with an excellent safety profile derived from animal and phase I human studies, Adrecizumab represents a promising candidate drug for the adjunctive treatment of sepsis. In this review, we first provide a brief overview of the currently available data on the role of adrenomedullin in sepsis and describe its effects on endothelial barrier function and vasodilation. Furthermore, we provide a novel hypothesis concerning the mechanisms of action through which Adrecizumab may exert its beneficial effects in sepsis.

Neostigmine pour tous ou monitoring pour tous ?
Catching a Unicorn: Neostigmine and Muscle Weakness—Not Neostigmine for All, but Quantitative Monitoring for Everyone!
Stephanie Phillips, B.Med., F.R.C.A., F.A.N.Z.C.A.; Paul A. Stewart, M.B., B.S., F.A.N.Z.C.A.
http://anesthesiology.pubs.asahq.org/article.aspx?articleid=2688287
Anesthesiology 8 2018, Vol.129, 381-382. doi:10.1097/ALN.0000000000002295
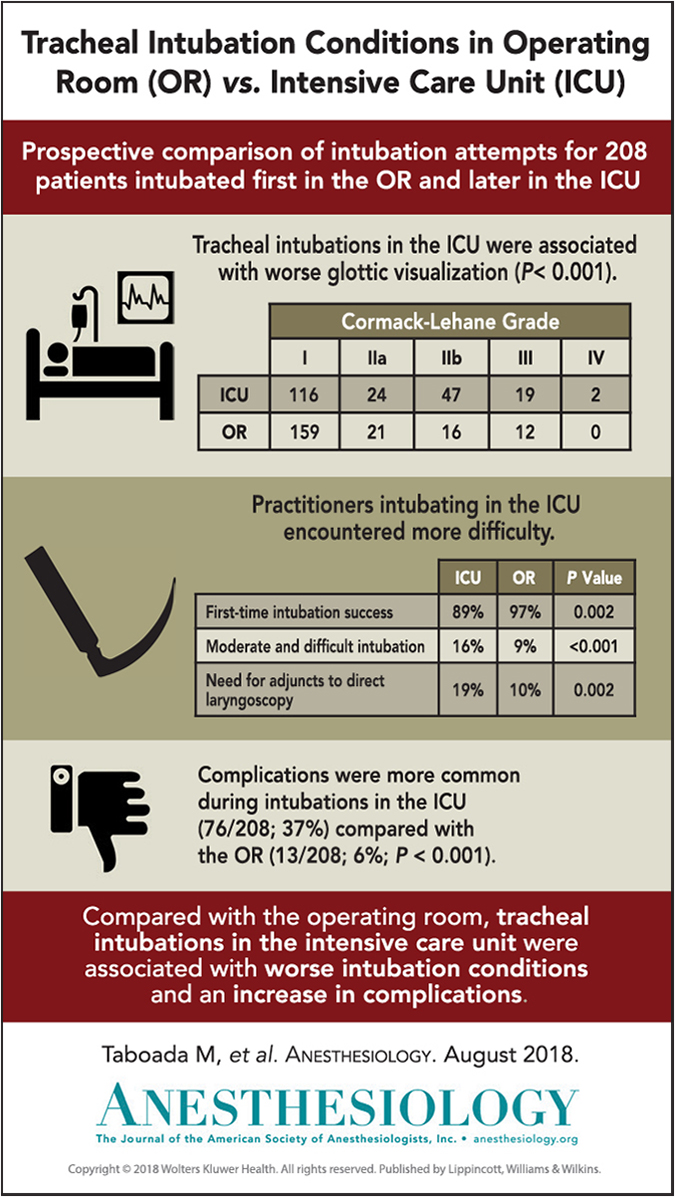
Intubation plus difficile en réanimation qu’au bloc opératoire…chez les mêmes patients malgré des anesthésistes aussi expérimentés !
Comparison of Tracheal Intubation Conditions in Operating Room and Intensive Care Unit: A Prospective, Observational Study
Manuel Taboada, et al., Anesthesiology, 2018
http://anesthesiology.pubs.asahq.org/article.aspx?articleid=2682493
doi:10.1097/ALN.0000000000002269
Abstract
Background: Tracheal intubation is a common intervention in the operating room and in the intensive care unit. The authors hypothesized that tracheal intubation using direct laryngoscopy would be associated with worse intubation conditions and more complications in the intensive care unit compared with the operating room.
Methods: The authors prospectively evaluated during 33 months patients who were tracheally intubated with direct laryngoscopy in the operating room, and subsequently in the intensive care unit (within a 1-month time frame). The primary outcome was to compare the difference in glottic visualization using the modified Cormack-Lehane grade between intubations performed on the same patient in an intensive care unit and previously in an operating room. Secondary outcomes were to compare first-time success rate, technical difficulty (number of attempts, operator-reported difficulty, need for adjuncts), and the incidence of complications.
Results: A total of 208 patients met inclusion criteria. Tracheal intubations in the intensive care unit were associated with worse glottic visualization (Cormack-Lehane grade I/IIa/IIb/III/IV: 116/24/47/19/2) compared with the operating room (Cormack-Lehane grade I/IIa/IIb/III/IV: 159/21/16/12/0; P < 0.001). First-time intubation success rate was lower in the intensive care unit (185/208; 89%) compared with the operating room (201/208; 97%; P = 0.002). Tracheal intubations in the intensive care unit had an increased incidence of moderate and difficult intubation (33/208 [16%] vs. 18/208 [9%]; P < 0.001), and need for adjuncts to direct laryngoscopy (40/208 [19%] vs. 21/208 [10%]; P = 0.002), compared with the operating room. Complications were more common during tracheal intubations in the intensive care unit (76/208; 37%) compared with the operating room (13/208; 6%; P < 0.001).
Conclusions: Compared with the operating room, tracheal intubations in the intensive care unit were associated with worse intubation conditions and an increase of complications.
Allergie présumée aux beta-lactamines : Evaluation et prise en charge des patients pour le bloc opératoire
Presumed β-Lactam Allergy and Cross-reactivity in the Operating Theater: A Practical Approach
Jeroen Hermanides, M.D., Ph.D.; Bregtje A. Lemkes, M.D., Ph.D.; Jan M. Prins, M.D., Ph.D.; Markus W. Hollmann, M.D., Ph.D.; Ingrid Terreehorst, M.D., Ph.D.
Anesthesiology 8 2018, Vol.129, 335-342. doi:10.1097/ALN.0000000000002252
Abstract
A β-lactam allergy is the most common suspected in-hospital drug allergy, with an incidence of 5 to 17% in hospitalized patients and up to 35% in the surgical population at the preoperative assessment clinic.1–5 Thus, the team in the operating theater will be confronted with these patients when perioperative antibiotic prophylaxis is needed. Frequently, the consequence of a presumed β-lactam allergy is that all β-lactam antibiotics are avoided, because of the possibility of cross-reactivity, and an alternative antibiotic, e.g., clindamycin, vancomycin, or ciprofloxacin, is prescribed.1 This may be a short-term risk-avoiding strategy during surgery, but the long-term consequences are overuse of these agents and an increase in serious hospital infections by pathogens such as Clostridium difficile and vancomycin-resistant Enterococcus, with an accompanied rise in healthcare use and costs.4 In fact, the overuse of non–β-lactam antibiotics because of reported penicillin allergy has been labeled a public health problem.6–8 In this review, we provide an evidence-based and practical approach to patients with presumed β-lactam allergy admitted to the operating theater and give guidance on the selection of alternative antibiotics based on cross-reactivity patterns.
 Étiquettes :
Étiquettes :